
The Latest News in Diabetes: 10 Highlights from EASD 2019
By Jimmy McDermottKarena Yan
 By Jimmy McDermott, Karena Yan, Emily Fitts, Martin Kurian, and Albert Cai
By Jimmy McDermott, Karena Yan, Emily Fitts, Martin Kurian, and Albert Cai
The diaTribe team was in Barcelona for the 55th Annual Meeting of the European Association for the Study of Diabetes. Check out our biggest highlights from the conference!
1. SUSTAIN 8 Results: Ozempic Shows Greater A1C Reduction and Weight Loss Than Invokana
This trial compared the A1C reduction and weight loss of Ozempic (a once-weekly injectable GLP-1 agonist) and Invokana (a daily pill SGLT-2 inhibitor). The study showed that:
-
Ozempic lowered A1C by 1.5 percentage points and Invokana lowered A1C by 1.0 percentage points (from an average starting A1C of 8.3%);
-
Ozempic resulted in a weight loss of 11.7 pounds (5.4 kg) and Invokana resulted in a weight loss of 9.3 pounds (4.2 kg) (from a starting weight of about 200 pounds or 90 kg); and
-
Ozempic helped more people reach the American Diabetes Association’s (ADA) A1C target of 7% (66% reached this target with Ozempic vs. 45% of people with Invokana).
Overall, the SUSTAIN 8 results show that both GLP-1 agonists and SGLT-2 inhibitors result in weight loss and A1C reduction. In addition, other studies have shown that these drugs can improve heart and kidney health – see more on this below!
2. Farxiga Treats Heart Failure in People with and without Type 2 Diabetes – Results from the DAPA-HF trial showcased the heart health benefits of SGLT-2 inhibitor Farxiga (spelled Forxiga in Europe) in people with and without type 2 diabetes.

Farxiga is now the first SGLT-2 inhibitor to show use as a treatment for heart disease and to demonstrate beneficial effects in people without diabetes. Results of this trial were first presented at the European Society of Cardiology – see more here!
3. DPP-4 Inhibitor + Metformin Combination Drug Slows Progression of Type 2 Diabetes Compared to Metformin Alone
The VERIFY study investigated the benefits of a combination drug – metformin combined with DPP-4 inhibitor (Galvus) in a single pill – versus metformin taken alone. The study compared the impact of the treatments on the delay or prevention in the rise of A1C among 2,000 people recently diagnosed with type 2 diabetes.
The combination drug delayed the rise in A1C to above 7% by 26-months compared to metformin alone (62 months versus 36 months). Treatment with the combination drug also delayed the requirement for insulin therapy.
This study shows that a metformin and DPP-4 inhibitor combination therapy is beneficial compared to metformin alone at the beginning of drug treatment for type 2 diabetes. By using two drugs at once, combination drugs can target multiple mechanisms within the body and lead to a greater protection of insulin producing beta cells.
4. CONCLUDE: A Study Comparing Hypoglycemia with Tresiba vs. Toujeo

CONCLUDE, a trial comparing next-generation basal insulins Tresiba and Toujeo for type 2 diabetes, showed no differences in the overall amount of hypoglycemia (or low blood sugar). The study did confirm that both of these next-gen basal insulins are beneficial: Tresiba and Toujeo lowered A1C from an average above 8.5% to 7.0% in just 24 weeks.
Of note, other trials have shown that these next-generation basal insulins reduce hypoglycemia in comparison to “first generation” basal insulins (DELIVER 2 and SWITCH 2 in 2017) but have similarly not identified meaningful differences in reduction of overall hypoglycemia between the two next-gen insulins (BRIGHT study at ADA 2018).
It is exciting to see that this study used hypoglycemia as the primary endpoint rather than A1C (what many studies use), which is a big step in the right direction in evaluating the daily reality of diabetes. Check out diaTribe’s resources to learn more about the Beyond A1C movement and the importance of measuring time-in-range.
5. CAROLINA Finds No Differences Between Tradjenta and Glimepiride Heart Health Outcomes
The CAROLINA study demonstrated that the DPP-4 inhibitor Tradjenta (linagliptin) and the sulfonylurea glimepiride are equally safe for the heart in people with type 2 diabetes. This is an important finding because previous studies have suggested that sulfonylureas may be unsafe for the heart. The FDA currently has a product-label warning for heart-related death for all sulfonylureas.
While these results presented at EASD were no different from those presented at ADA, the commentary from Professor Philip Home at EASD was impactful. He gave glowing praise for the study, which he found to be both well-conducted and much-needed. Not only did the study use a rather ethnically and geographically diverse group (making the results easier to apply to the general population) but it also countered the common belief held for over 40 years that SUs are unsafe for the heart. Additionally, these results can give peace of mind to the many people with diabetes who are using these drugs.
However, sulfonylureas are known to carry a greater risk of hypoglycemia than other type 2 diabetes medications. CAROLINA confirmed increased hypoglycemia with glimepiride, showing a 77% increased risk of hypoglycemia overall; 38% of those on glimepiride experienced hypoglycemia, compared to 11% of those on Tradjenta. Looking more closely, glimepiride had an 85% increased risk of severe hypoglycemia and a 93% increased risk of hospitalization for hypoglycemia. This alone is reason to avoid glimepiride if at all possible. If not, we encourage people to check blood glucose levels as frequently as possible.
6. SGLT-2 Inhibitor Farxiga Improves Symptoms and Quality of Life in People with Heart Failure
In one of the most packed sessions of the second day, Dr. Mikhail Kosiborod and Dr. Michael Nassif revealed new results from the DEFINE-HF trial, showing that 12 weeks of treatment with Farxiga improved scores on the Kansas City Cardiomyopathy Questionnaire (KCCQ) compared to placebo for people with and without type 2 diabetes. The KCCQ is a questionnaire for people with heart failure – the questionnaire measures symptoms, function, and quality of life. We were pleased to see a study specifically aimed at understanding the perspective of people with heart failure. As Dr. Kosiborod emphasized, one of the goals for treating patients with heart failure is to improve health status, including symptom burden, physical limitations, and quality of life.
7. SGLT-2 Inhibitor for Type 1 Diabetes: Why is There a BMI Cut-Off?
In May 2019, the European Medicines Agency (EMA) approved Zynquista, an SGLT-1/2 dual inhibitor, for people with type 1 diabetes and a body mass index (BMI) above 27. At EASD 2019, Dr. Thomas Danne shared an analysis comparing Zynquista in people with type 1 diabetes with a BMI greater than 27 versus those with a BMI less than 27. The analysis showed that for those with a BMI greater than 27, Zynquista resulted in:
-
Greater A1C lowering;
-
Larger improvements in time-in-range; and
-
Slightly lower rates of diabetic ketoacidosis (DKA).
It is likely that the EMA proposed the BMI cutoff in light of these greater benefits and reduced risk of DKA. Earlier this year, the FDA decided not to approve Zynquista for people with type 1 diabetes.
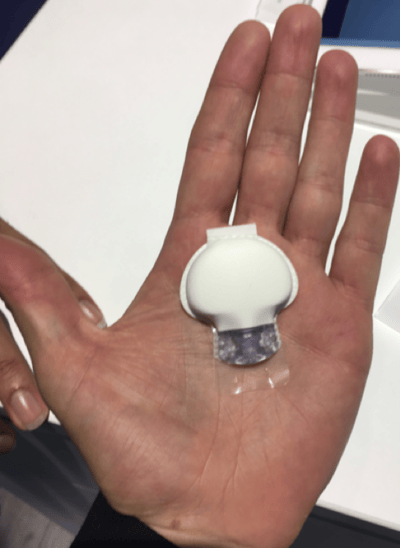
8. Medtronic Announces New Professional CGM “Envision Pro”

Medtronic announced that it received European approval (formally called “CE Mark” approval) for “Envision Pro” – its new professional CGM for type 1 or type 2 diabetes – which will be available in Europe and the Middle East in the fall of 2019. There are no plans for Envision Pro to be launched in the US.
The new professional CGM has many exciting features, including:
-
Fully-disposable – Envision Pro can be easily discarded after use.
-
No-calibrations – No fingersticks needed!
-
Bluetooth – CGM data is sent directly to the Envision Pro app via Bluetooth and then relayed to CareLink, which is a program that provides information and insights to clinicians. This means people don’t have to return the transmitter to the clinic at the end.
-
Blinded – While wearing Envision Pro, people do not see their glucose readings.
-
Seven-day-wear – People wear Envision Pro for one week.
Professional CGM allows a doctor or diabetes specialist to get continuous glucose data over the duration of the CGM (in this case, seven days). The data helps people with diabetes and their doctor to personalize treatment and figure out ways to improve glucose management. Since Envision Pro is fully disposable, does not require fingerstick calibrations, and automatically uploads data to the CareLink platform, it does not require users to return to the clinic after use.
Abbott and Dexcom also have professional CGM systems, called Abbott FreeStyle Libre Pro and Dexcom G4 Platinum. Dexcom’s newer G6 Pro is currently under FDA review. Here’s a comparison of the three systems:
|
Medtronic Envision Pro |
Abbott FreeStyle Libre Pro (approved in 2016) |
Dexcom G6 Pro (under FDA review; 2020 launch expected) |
|
|
Wear time? |
7 days |
14 days |
10 days |
|
Requires fingerstick calibration? |
No |
No |
No |
|
Fully disposable? |
Yes |
Yes |
Yes |
|
MARD (measure of accuracy based on how far the readings are from the true value, on average) |
11.0% |
12.3% (least accurate) |
9.0%* (most accurate) |
|
Does CGM data upload to the app via Bluetooth? |
Yes Data uploads automatically to CareLink |
No Person must come to clinic to have sensor downloaded |
Yes Data uploaded to Dexcom Clarity (via G6 app) or stored on receiver |
|
Is data blinded or visible in real-time for the user? |
Blinded Only |
Blinded Only |
Blinded and Real-Time modes |
*Accuracy, or MARD, for Dexcom G6 Pro assumes that it will use the same sensor and algorithm as the Dexcom G6.
9. Dexcom Adds Insulin Smart Pen Data to Clarity App for Better Decision Support
Dexcom’s Clarity is now integrating Companion Medical’s InPen data for a combined view of insulin data and CGM data.
Clarity gives Dexcom users information about their recent CGM trends and statistics, including setting a daily time-in-range goal, notifying users of their “best day” over the past week, and calculating users’ estimated A1C based on 14 days of CGM data (called “Glucose Management Indicator”). Companion Medical’s InPen is a reusable, Bluetooth-enabled smart insulin pen that automatically records the amount of mealtime insulin a user injects and the time of injection. For now, InPen uses cartridges of U-100 Novolog and Humalog.
.png)
Combining insulin data and CGM data helps support decision-making, since it adds more context to glucose levels measured by CGM alone.
.png)
Looking ahead, Dexcom is continuing to develop tools to improve decision support, such as a “CGM-informed” bolus calculator, better hypoglycemia prediction, “on-demand” sleep and exercise advice, and more glucose control assessment. Dexcom is planning to launch the “CGM-informed” bolus calculator before the G7 launch (currently targeted for late 2020-early 2021), which will help people who inject insulin figure out how much to bolus based on their continuous glucose data.
10. Dr. Rich Bergenstal Urges for Greater Focus on Outcomes Beyond A1C: CGM, Time-in-Range, and AGP
Dr. Rich Bergenstal expertly advocated for diabetes care to focus on outcomes beyond A1C, particularly by using CGM data to measure time-in-range. EASD 2019 has been packed with discussions on time-in-range and CGM use, coming up in some form in almost every session. This increased focus follows a global consensus on targets for time-in-range and an update to ADA’s Standards of Care that included the agreed upon targets and CGM metrics.

A1C has long been the “gold standard” for diabetes care in clinical and regulatory settings due to its correlation with long-term complications, but Dr. Bergenstal is pushing to validate time-in-range as the next “gold standard.” In 2018, Dr. Bergenstal and others published a paper in Diabetes Care that linked time-in-range with complications, including retinopathy and microalbuminuria. In his presentation, Dr. Bergenstal highlighted that A1C has significant limitations, especially because it does not identify hypoglycemia or glucose variability. Read more on why A1C alone is not enough here.

Looking to the future, Dr. Bergenstal called for research on the correlation between time-in-range and long-term outcomes using CGM data, saying “CGM will never win the day if you are not convinced that it is related to long-term complications.” In the August 2019 Stand of Care updates, ADA also recommended use of the one-page AGP (ambulatory glucose profile), which Dr. Bergenstal called “the EKG for glucose management” due to the comprehensive and concise nature of both reports. AGPs (as well as EKGs) provide answers to the two main questions in glucose management with the output of metrics and a profile: “Is there a problem?” and “Where is the problem?”
In conclusion, Dr. Bergenstal shared two acronyms that he uses to help people understand their AGP (or CGM) profile: MGLR (more green, less red) and FNIR (flat, narrow, and in range).
For a comprehensive review of time-in-range, see our resource page here.






