Rules of Engagement for Basal Insulin Adjustment (Or, Avoiding Basal Blunders!)

It seems like there are rules for everything these days. Rules for dating. Rules for e-mail etiquette. Even rules for raising kids. And so, it only seems fair that I get to create some rules of my own.
Since nothing drives me battier than people who make ill-conceived changes to the basal settings on their insulin pumps, I think I’ll take this opportunity to offer some experience-laden insight on the subject.
Before getting down to rule-writing, it should be understood that the role of basal insulin is to match the liver’s normal output of glucose, thus keeping blood glucose levels steady between meals and during sleep. The only true way to determine whether the existing basal settings are working properly is to perform fasting tests at each phase of the day and night. During a basal test, the only thing raising blood glucose should be the liver, and the only thing lowering it should be basal insulin. All other influences (food, bolus insulin, exercise activity, major stress, hormonal changes) need to be eliminated.
Typically, a basal test can begin approximately four hours after the last meal and bolus, with the preceding meal being relatively healthy (not too much fat). During the test, blood glucose levels are taken every hour or two, or a CGM can be used to collect the information. The test is only stopped if the blood glucose rises much too high or drops too low. As long as it stays within a reasonable range, the test should continue. If the blood glucose varies by less than 30 mg/dl (1.7 mmol/l) during a basal test, we usually consider it steady enough to verify the basal setting during that time. Otherwise, changes are probably in order.
When making basal changes, it’s important to keep the following “rules of engagement” in mind:
1. Make basal changes before blood glucose starts to rise or fall.
Having diabetes teaches us that we need to plan ahead. The so-called “rapid-acting” insulin we use takes 60 to 90 minutes to peak, and three to four hours to just about finish working. Thus, increasing (or decreasing) a basal rate at 6 PM is not going to affect the blood glucose at 6 PM. My preference for most children is to adjust basal rates starting one hour prior to observed blood glucose changes, and two hours prior for most adults. For example, if a child’s blood glucose is dropping from 3 to 6 AM, I would recommend a basal reduction from 2 to 5 AM. If an adult’s blood glucose is rising from 4 to 10 PM, I would recommend an increase from 2 to 8 PM.
2. Adjust in appropriate increments.
Making tiny, infinitesimal basal insulin adjustments in someone on very large doses is like trying to take down a charging rhino with a water pistol. Likewise, making relatively large changes in someone on very small doses is like shooting a fly with a bazooka. The amount of the basal change needs to reflect both the magnitude of the observed blood glucose change and the individual’s sensitivity to insulin. The chart below should serve as a good starting point:

3. Adjust on the hour.
This is simply a way to keep things tidy. Remember, basal insulin is composed of tiny pulses of rapid-acting insulin delivered every couple of minutes. As I mentioned earlier, each pulse takes 60 to 90 minutes to peak and three to four hours to finish. Adjusting basal rates on the half-hour will not produce a more rapid or dramatic change to the level of active insulin than making adjustments on the hour. However, adjustments on the half-hour can complicate the evaluation process, since a certain rate is delivered for the first half of the hour, and a different rate for the second half. So keep it simple -- make your basal setting changes on the hour.
4. Maintain the “integrity” of the program.
When setting up a 24-hour basal program, our objective is to mimic normal physiology as closely as possible. A healthy pancreas secretes basal insulin in a circadian pattern, based mainly on how other hormone levels vary during the course of a full day. More basal insulin is produced at certain hours, less at others. There tends to be one “peak” and one “valley” – not multiple peaks and valleys. A basal program that includes multiple peaks and valleys is almost always incorrect, or at least compensating for some other aspect of the insulin program that is not set up properly. For example, consider this pattern:
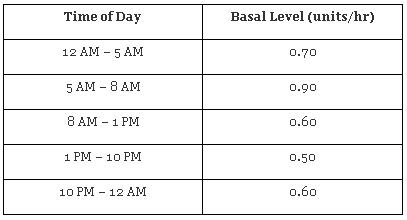
This pattern has one “peak” (5 to 8 AM) and one “valley” (1 to 10 PM). It has integrity, as far as basal programs go. Now consider this pattern:
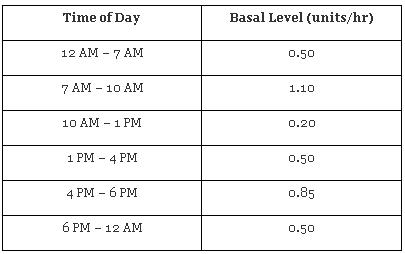
This program has two peaks (a big peak from 7 to 10 AM, and a smaller peak from 4 to 6 PM). Given that the basal rate is 0.50 units/hr continuously from 1 PM until 7 AM except for those two hours in the late afternoon, something may be set inappropriately. Perhaps it is compensating for an afternoon snack that is not covered sufficiently with a bolus.
When making basal adjustments based on fasting basal tests, it is sometimes necessary to extend basal segments beyond the scope of the time that was tested in order to prevent a “choppy” program. For example, if a person with the following basal program tests his or her morning basal rate by skipping breakfast and finds that (s)he is dropping from 8 to 11 AM, (s)he might consider decreasing his or her basal right up to 1 PM in order to create a program that has a logical 24-hour flow.

Note that lowering the basal rate from 7 AM to only 10 AM (as indicated by the fasting test) would create a multi-peak, multi-valley basal pattern. Extending the decrease to 1 PM keeps the program smooth, with one peak and one valley. This is the “art” of basal insulin adjustment!
5. Consider the norms (but don’t live by them).
There are all sorts of “standards” to judge a person’s basal program. People who still produce some of their own insulin tend to have flatter basal patterns than those who make no insulin at all. For most people, 40-50% of the total insulin for the day is basal insulin. And young people (during growth years) tend to have prolonged peaks through the night rather than a pronounced peak in the early morning, also known as a dawn phenomenon (see graph below).
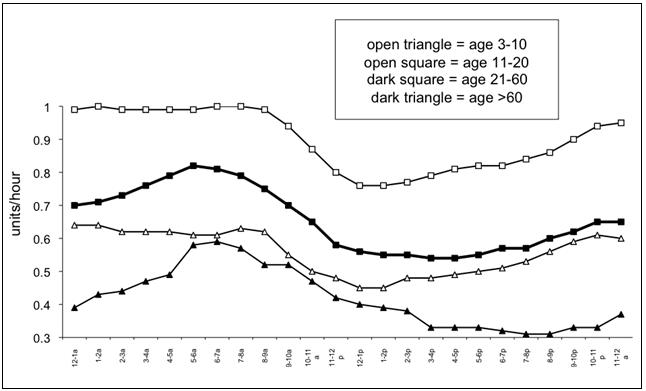
However, please keep in mind that these standards are based on averages taken from large groups of people. If we know anything about diabetes, it is that every person’s needs are unique. Trying to make your basal program conform to a preset standard may be like trying to squeeze the proverbial square peg into the round hole.
When it comes to basal insulin, don’t take shortcuts. Go through the basal testing and find out what your needs really are. It is well worth the effort.
Fine-tuning basal insulin doses can be complex. Don’t hesitate to reach out to a member of your health care team who specializes in this sort of thing.
Gary Scheiner, MS, CDE is a diabetes educator with a private practice (Integrated Diabetes Services) and author of “Think Like A Pancreas: A Practical Guide to Managing Diabetes With Insulin.” He has had type 1 diabetes for 25 years. He and his team offer diabetes management consultations via phone and internet to insulin-users throughout the world. For more information, call (877) 735-3648 or e-mail gary@integrateddiabetes.com.