Study Compares MiniMed 780G and MiniMed 670G Algorithms

By Albert Cai
A new study in adolescents and young adults with type 1 diabetes directly compared two automated insulin delivery algorithms. Medtronic’s newer Advanced Hybrid Closed Loop (built into the MiniMed 780G system) improved glucose management more than the MiniMed 670G, though both systems showed impressive increases in Time in Range for this population. Ultimately, the 670G gave users over an hour and a half more time in range each day, while the 780G gave wearers over two hours every day in range!
Two Medtronic automated insulin delivery algorithms, the Advanced Hybrid Closed Loop and the MiniMed 670G, were recently compared in a cross-over study, allowing 113 participants to use both algorithms. Results from the study were published in the medical journal The Lancet. Notably, the study tested this technology in adolescents and young adults with type 1 diabetes – a group for which diabetes management is notoriously challenging. View our resources for adolescents with diabetes here.
For an introduction to automated insulin delivery (AID), check out our piece on current and coming-soon AID systems in 2021.
What is the MiniMed 670G?
The MiniMed 670G is an AID system that has been available since spring 2017 – it was the first system ever to “close the loop.” The system includes the MiniMed 670G pump, the Guardian Sensor 3 continuous glucose monitor (CGM), and an automated insulin adjustment algorithm. The algorithm adjusts basal insulin delivery every five minutes based on CGM readings, and a target of 120 mg/dl.
What is Advanced Hybrid Closed Loop?
Advanced Hybrid Closed Loop (AHCL) is Medtronic’s next-generation AID algorithm. The AHCL algorithm is used in Medtronic’s MiniMed 780G system, which is currently available in at least twelve countries in Europe. While it is not yet available in the US, Medtronic hopes to launch the 780G in the US this spring. In addition to automatic basal rate adjustments, the AHCL algorithm can also deliver automatic correction boluses and has an adjustable glucose target that goes down to 100 mg/dl. This is big news because many people using closed loop do not want to target the higher 120 mg/dl, even as a safety measure. The 780G algorithm is designed to have fewer alarms and even simpler operation than the MiniMed 670G system.
What was the study?
The newly published FLAIR (Fuzzy Logic Automated Insulin Regulation) study was conducted over six months across seven diabetes centers (four in the US, two in Europe, and one in Israel). The study enrolled 113 adolescents and young adults (ages 14-29) with type 1 diabetes. The study sample is notable, because teens and young adults with type 1 diabetes have the highest average A1C levels of any age group.
At the beginning of the study, participants performed their usual diabetes management routine for two weeks to establish their baseline glucose levels. Half of the group was then randomly assigned to use the MiniMed 670G system, while the other half of the group used the same pump and CGM, but with the new AHCL algorithm. After three months – the halfway point of the study – the two groups “crossed over,” switching to the opposite technology.
What were the results?
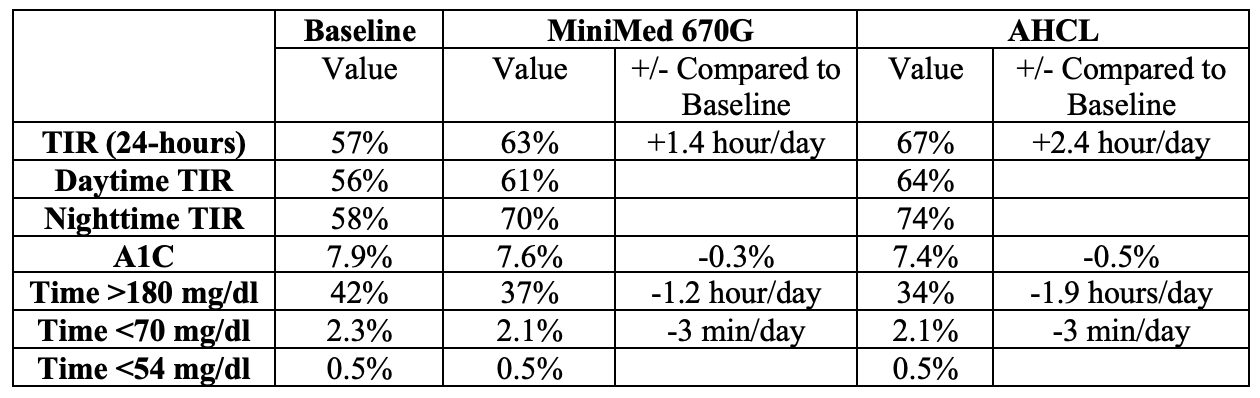
Nearly every measure of glucose management favored the AHCL period over the MiniMed 670G:
- Compared to baseline, participants reduced time spent above 180 mg/dl by 1.2 hours per day when using MiniMed 670G and 1.9 hours per day when using AHCL.
- Time in Range (TIR, time between 70-180 mg/dl) improved from a baseline of 57% to 63% using Minimed 670G and to 67% using AHCL.
- Time spent below 70 mg/dl fell 0.2% of the time. While those 28 minutes a day may not be statistically significant – and time in severe hypoglycemia, or below 54 mg/dl, did not increase from baseline when using either algorithm – many people with diabetes would benefit from that additional half hour in range.
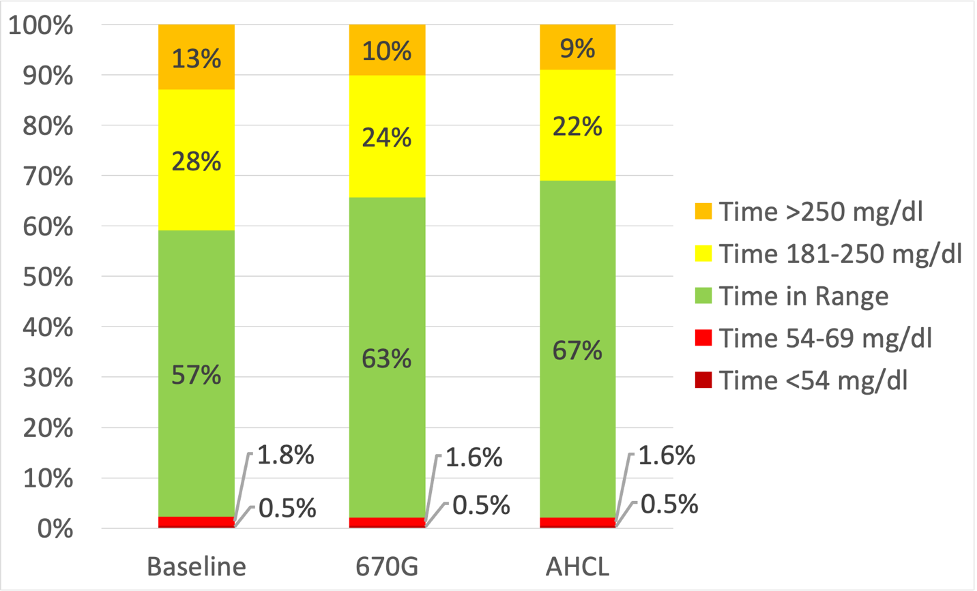
The graph below shows the time spent in glucose ranges during baseline, MiniMed 670G, and AHCL periods. For both algorithms, the Time in Range increase from baseline was significant – use of either AID system led to at least 14 hours more each week spent in range. Nevertheless, we also point out, of course, that the group (again, the group that has the most challenges of any age group managing diabetes) still experienced a fair amount of time above 250 mg/dl. This is another reason for healthcare professionals and people with diabetes to think about the “whole person” when considering diabetes management, and another reason why we always recommend Adam Brown’s Bright Spots and Landmines for ways to improve diabetes management in terms of food, exercise, mindset, and sleep – it includes many strategies for people, especially teens and young adults, to use each day.
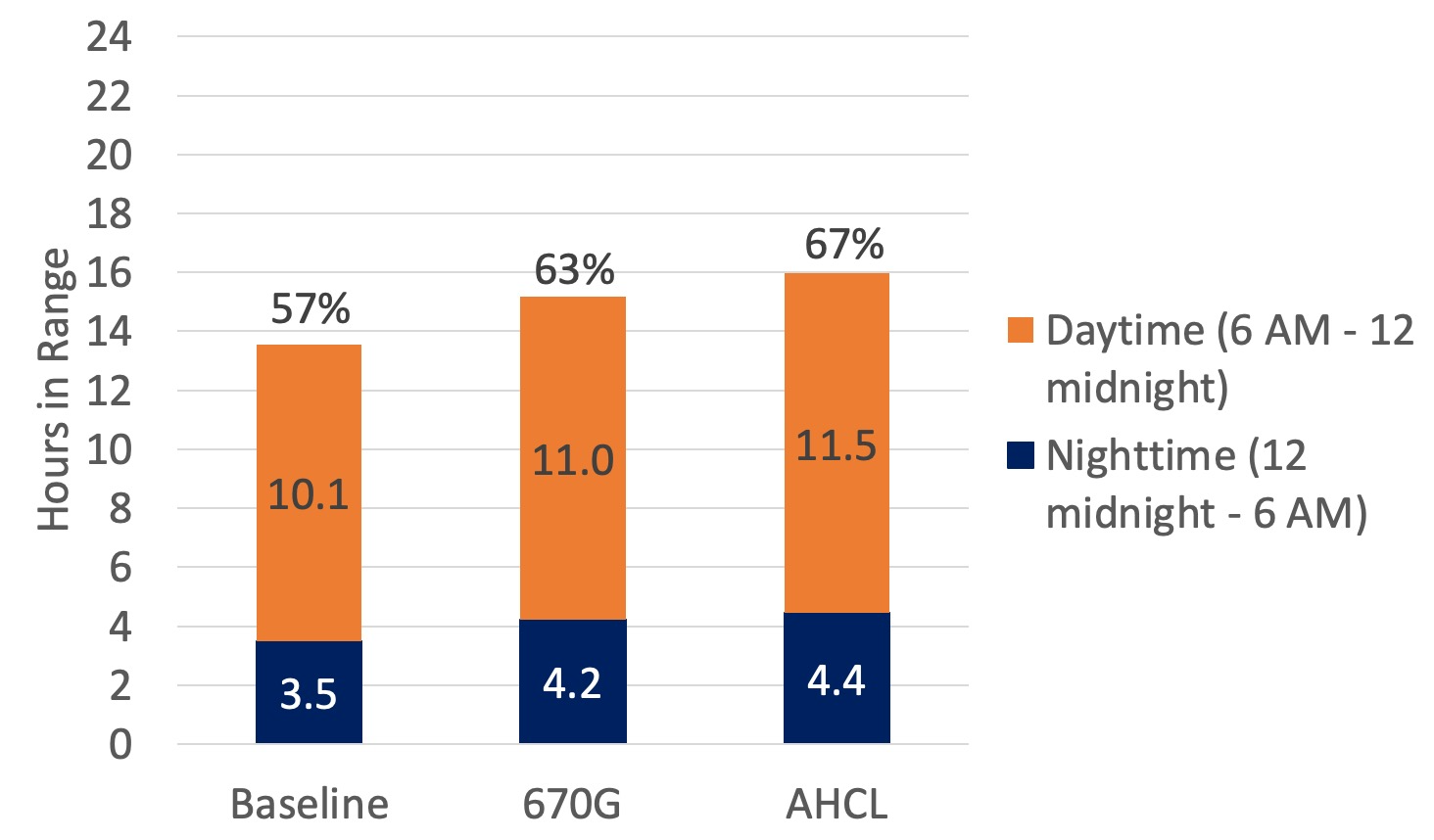
- The biggest Time in Range improvement came overnight (between midnight to 6am). During this six-hour overnight period, AHCL users spent an average of 4.4 hours in range (74% TIR), compared to 4.2 hours (70% TIR) for 670G, and 3.5 hours (58% TIR) during baseline. While the overnight Time in Range difference between AHCL and 670G may not seem large, it added up to nearly a 22-hour difference over the three-month the AHCL period.
- With daytime numbers, the average AHCL user spent 63 more hours (about 2.6 days) in range than the average 670G user in each three-month study period.
The graph below shows daytime and nighttime differences in time spent in range (70-180 mg/dl), and the data is included in a table at the end of this article. Better sleep the night before can also make diabetes management more effective during the day.
- Using MiniMed 670G drove an average A1C improvement from 7.9% to 7.6%, while AHCL use improved A1C from 7.9% to 7.4%.
Both systems showed extremely positive results and were found to be safe for use in young people with type 1 diabetes. The AID algorithms led to dramatic increases in Time in Range in a population that stands to benefit – over the course of a year, adolescents and young adults could spend more than ten additional days in range. The direct comparison between these two AID algorithms is highly informative – we hope to see similar trials in the future.