What are your “Diabetes Landmines?” The Seven Mistakes I Always Make and What I Learned Trying to Avoid Them

by Adam Brown
view an infographic summary of this article
twitter summary: Adam shares seven diabetes landmines – his mistakes that routinely lead to out-of-range blood sugars – and some solutions he’s been trying
short summary: In this article, I share my own “diabetes landmines”– seven small mistakes I seem to make again and again that “explode” into out-of-range blood glucose values. These include: overcorrecting low blood sugars with too many carbs; overcorrecting a high with too much insulin (“stacking”); snacking directly out of the package; eating when I am not hungry; eating too quickly or overeating; eating too close to bedtime; and not increasing my basal rate following a night of poor sleep or on a day with little exercise. I also identify some solutions I’ve been using to try to overcome these mistakes.
After writing my last column on the 22+ short-term factors that affect blood glucose, I wondered...
“Even though diabetes is very unpredictable, are there some consistent reasons why my blood glucose falls out of range?”
Yes. I call these my “diabetes landmines”– small mistakes I seem to make again and again that seem to “explode” into out-of-range blood glucose values. The list below highlights the seven mistakes I routinely make, and also details some solutions I’ve been trying out. Writing this list and the potential solutions was highly valuable for me; for the past few weeks, I’ve been more aware of my own “diabetes landmines” and have felt more equipped and motivated to avoid them. Try writing your own list along with some solutions, and email me at adam.brown(at)diaTribe.org or tweet me at @asbrown1 with what you find!
Mistake#1: Overcorrecting low blood sugars with too many carbs, only to go high afterwards. I consider myself someone with a lot of willpower, but with a blood sugar of 55 mg/dl, sometimes I just want to eat everything in sight.
Solution A: Having a single go-to correction for hypoglycemia. Though they’re not the greatest tasting treat, I know that one glucose tab (4 grams of carbs) raises my blood glucose by about 20 mg/dl. It’s predictable, and I know I won’t overeat glucose tabs. Other people I know use mini juice boxes, glucose gels, or packets.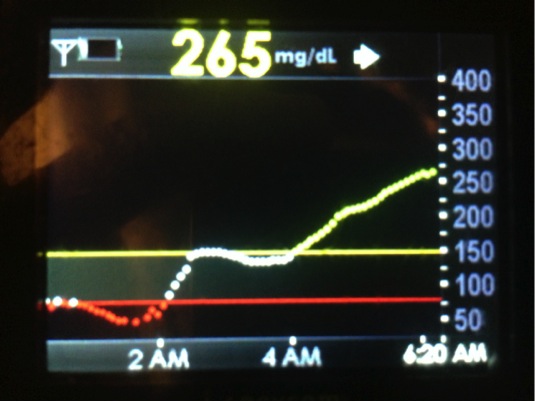
Solution B: Avoiding tempting foods as hypoglycemia treatment options. It’s deadly easy to use a low blood sugar as an excuse to overeat a food you would not normally consume. See the picture on the right – that blood sugar nightmare occurred after I stormed the fridge at 2 am and corrected a nighttime low using granola from a friend’s work event. The huge bowl was sitting in our fridge, and “I only had a little.” Bad idea! When I use low blood sugars as a justification to eat bad food, I always regret it.
Mistake #2: Taking too much insulin (“stacking”) when high, and then going low soon after. Rapid-acting insulin can sometimes feel so SLOW, especially if you wear CGM.
Solution A: Patience. I have to remind myself that in my body, rapid-acting insulin takes about 60-90 minutes to really start dropping my blood glucose and two to three hours to finish working. [Note these times vary from patient to patient and depending on the size of the bolus.]
Solution B: Use the bolus calculator to account for insulin on board. When I stack insulin, it’s because I’m taking too many manual boluses. Using my pump’s built-in calculator reminds me that there is still bolus insulin floating around my system. If you take injections, the Timesulin pen cap could be helpful; it is available in Europe and coming very soon to the US.
Solution C: Take walks to correct highs and minimize insulin intake. For a moderately high blood sugar (e.g., 180 mg/dl), I prefer a short walk to drop my glucose – it’s more predictable and often sufficient to bring me back down into range. Even if I only see a modest drop in blood sugar, I’m starting from a lower and safer base to correct from.
Mistake #3: Snacking directly out of the package. It’s amazing how quickly I can consume too much of any snack (especially salty options), just because there is a visible package on my pantry shelf and I can mindlessly pour a lot into my hands.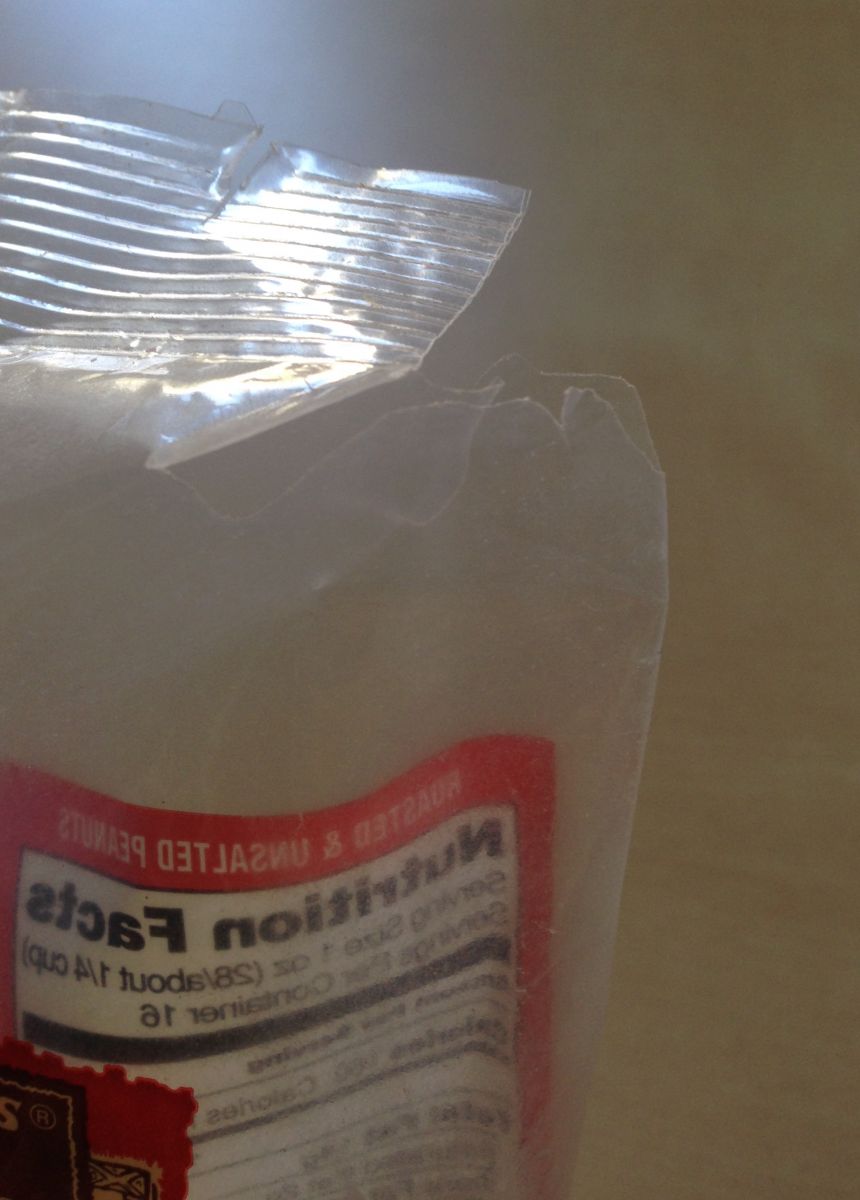
Solution A: Tearing a smaller hole in the package. I’ve been using scissors to cut a small triangle off the corner of snack packages. This strategy has proven very effective in cutting my consumption – it takes much more shaking, effort, time, and patience to get the same quantity of a snack out of the package.
Solution B: Always pouring snacks into a container instead of directly into my hand. Adopting a blanket, “No-eating-directly-out-of-the-package” policy has been somewhat helpful in curbing this bad habit. In addition to cutting small corners in packages (solution A), I have recently begun trying to force myself to find a bowl or Tupperware container to pour into. If I want more, I have to make the effort to return to the package and put more into the bowl.
Solution C: Stationing myself away from kitchen/snacks. Much of my snacking comes from being in the same room as food. Sitting in my living room or on the back patio, as well as hiding snacks out of sight, has been very helpful.
Mistake #4: Eating when I am not hungry. I do this all the time, particularly when I work from home at my kitchen table.
Solution A: Asking myself, “Am I hungry or just bored/tired/sensing food?” It’s almost always that I’m around food, and my brain is telling me to eat it, even though I don’t have the sensation of hunger.
Solution B: Drinking water or tea. Often, I can overcome a desire to eat by drinking water or tea. I’ve become a big fan of loose-leaf hot green tea over the past few years, which fills me up without any calories.
Solution C: Setting a hard-and-fast rule. I’ve been experimenting with the following black-and-white approach: at least three hours must pass between snacks/meals (unless I am low). This prevents me from snacking indiscriminately just because food is around.
Mistake #5: Eating too quickly or overeating. I’m a flagrant offender of this one, particularly if I’m low and/or haven’t eaten in many hours. This is a particularly challenging in type 1 diabetes, since the appetite-suppressing hormone amylin is missing.
Solution A: Eating slower than people I’m eating with. When I’m eating with at least one other person, it’s easy to see how relatively fast I’m finishing my food. I’ve been aiming to eat slower than my meal partners.
Solution B: Eating with chopsticks. I’ve been experimenting with this on and off for years and love how much it slows down my eating. The hard part is remembering to grab them out of my kitchen drawer.
Solution C: Adding more vegetables. For a low-calorie, low glycemic-impact way to fill up, few things beat vegetables. I’ve bought organic frozen vegetables from Trader Joe’s since college – they won’t spoil, are fairly inexpensive, and many experts say they are just as nutritious as buying fresh.
Mistake #6: Eating too close to bedtime. Often, I’ll eat a low-carb meal close to bedtime, go to sleep with an in-range blood sugar, and wake up in the middle of the night at 190 mg/dl.
Solution A: Eating more calories earlier in the day. When I eat late at night, it’s often because I’ve barely eaten anything all day, or grazed on snacks and not eaten proper meals. I like the old saying, “Breakfast like a king, lunch like a prince, and dinner like a pauper.”
Solution B: Avoiding high-fat meals and snacks within three hours of bedtime. I always overeat nuts too close to bedtime, which provokes insulin resistance and a consequent slow and steady rise in blood glucose once I go to bed. See factor #2 here for more detail on why high-fat meals increase blood glucose.
Mistake #7: Not increasing my basal rate following a night of poor sleep or on a day with little activity. My basal rate is set to keep me in range when I’ve gotten at least seven hours of sleep and I’m fairly active (>10,000 steps in a day or some vigorous exercise). If I fall short of either of these goals – typically when traveling – I often need to increase my basal rate to stay in my target zone.
Solution A: Increasing my daytime basal rate by 10-30%. This is a huge advantage of wearing an insulin pump, since it requires just a few button pushes.
Solution B: Getting more sleep. Easier said than done, of course, but hugely important for better blood sugars, as I wrote in a previous Adam’s Corner. I aim for more than seven hours of sleep and feel most energetic with more than eight hours.
Solution C: Sneaking in activity. I always forget that even a little activity makes a difference. Kelly and I have been known to walk up and down the aisle of an airplane to get steps in while traveling. It’s really fun when we’re flying together, although passengers have been known to get annoyed. I’ve found that even 10 minutes on a stationary bike at a basement hotel gym is better than nothing. When on the road, I also really like the Seven Minute Workout (iPhone and Android), which requires no equipment and can be done in hotel rooms.
I would strongly encourage anyone with diabetes to make a personal list of “diabetes landmines” that seem to lead to out-of-range blood sugars. Just as I did above, try to identify some potential solutions to avoid these scenarios in the future. If nothing specific comes to mind, try this: each time you see an out-of-range blood sugar over the next seven days, try to pinpoint a reason why it occurred. At the end of seven days, can you spot any patterns?
Email me at adam.brown(at)diaTribe.org or tweet me at @asbrown1 #diabeteslandmine with what you find!
Download your own infographic of the article here:
[Editor’s Note: Adam is a patient with diabetes and not a health care provider. Please consult with your health care provider before making any changes to your diet, insulin, or medication regimen.]
Adam is Senior Editor of diaTribe and Chief of Staff/Head, Diabetes Technology at Close Concerns. He is a graduate of the University of Pennsylvania and serves on the board of the San Francisco branch of JDRF. He was diagnosed with type 1 diabetes at the age of 12, and has worn an insulin pump for the last 12 years and a CGM for the past four years. Adam is passionate about exercise, nutrition, and wellness and spends his free time outdoors and staying active. He can be reached at adam.brown(at)diatribe.org or @asbrown1 on twitter.