2019 JDRF Mission Summit Highlights Hope for a Cure and New T1D Treatments

By Jimmy McDermott, Peninah Benjamin, Martin Kurian, and Kelly Close
Learn more about JDRF’s efforts in finding a cure for type 1 diabetes and read highlights from experts’ discussions on SGLT inhibitors in type 1 and Beyond A1C
JDRF recently held its annual Mission Summit in Naples, Florida. The agenda focused on cures for type 1 diabetes (note – plural!), the potential for SGLT inhibitors (Jardiance, Farxiga, Invokana, Zynquista, etc.) in type 1, and the Beyond A1C movement. Notably, JDRF invests two-thirds of its research and development budget on cure efforts and is in the midst of multiple meetings with the US FDA and insurance companies to speed this on. Read more for highlights on approaches to cures as well as a most valuable conversation with Yale pediatric endocrinologist Dr. Jennifer Sherr, who also has type 1 diabetes!
Roadmap to a Cure
JDRF leadership outlined the need for a cure roadmap, just like the one used to develop automated insulin delivery (aka “artificial pancreas” or “closed loop” systems). JDRF’s Chief Mission Officer Dr. Aaron Kowalski looked back to 2009, when he published a landmark paper that laid out key stepping stones to developing commercially available automated insulin delivery systems – e.g., suspending insulin delivery when blood sugars are already low (MiniMed 530G), predictively suspending insulin before lows (MiniMed 640G, Tandem Basal-IQ), hybrid closed loop (MiniMed 670G), and fully closed loop. This roadmap provided “specificity and clarity” to guide research, companies, and discussions with the FDA. Dr. Kowalski argued that this kind of “crystal clear” roadmap is now needed in type 1 diabetes cure research – beta cell therapy (replacing the cells in the pancreas that produce insulin) and immunotherapy research. Dr. Kowalski believes that “cures” will take many forms and progress in steps over time – just like automated insulin delivery.
For instance, Dr. Sanjoy Dutta, Associate Vice President of Research and International Partnerships at JDRF, mentioned a first-generation product for replacing beta cells – the idea would be to provide six months of independence from insulin to start. This is not a full “cure,” but it would be a valuable leap in progress nonetheless. Early beta cell replacement takes the form of implanting a device that contains cells designed to mature into insulin-secreting beta cells. In addition to ViaCyte and Sernova, there is a third (unnamed) research group tackling this product.
Dr. Kowalski expressed excitement on the state of research for a cure: “We’re at a pivot point …it’s about us filling in the gaps and driving it to the finish line.” Progress on curing type 1 diabetes has had many disappointments, though Dr. Kowalski emphasized JDRF’s commitment and the exciting stage of early research.
Reducing the Burden of Type 1 Diabetes: A Conversation with Dr. Sherr
We enjoyed a conversation between JDRF’s Dr. Aaron Kowalski and Yale’s Dr. Jennifer Sherr, who is a pediatric endocrinologist with type 1 diabetes.
On SGLTs in type 1:
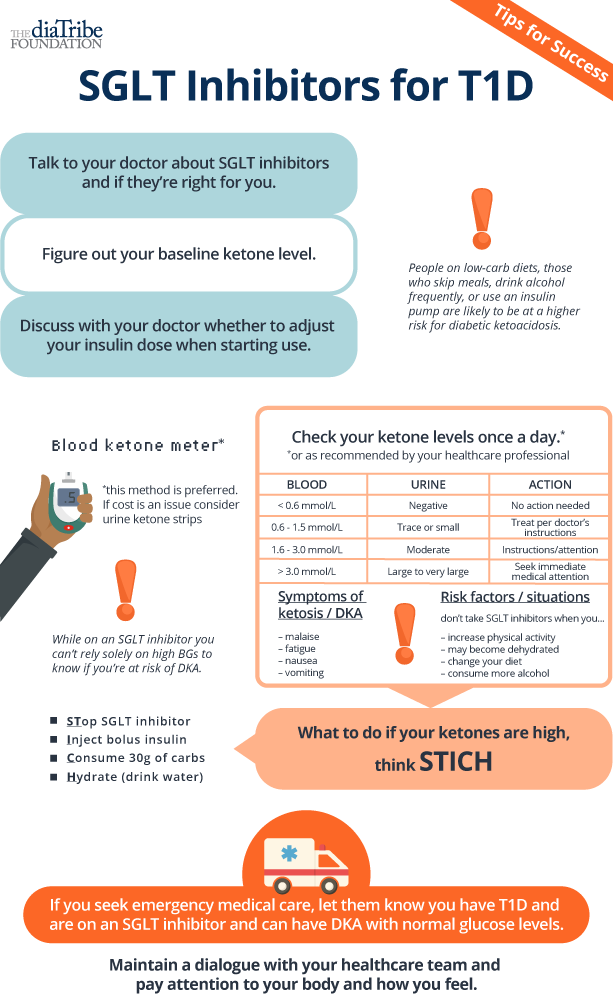 On January 17th, an FDA Advisory Committee vote tied 8-8 on whether or not to approve Zynquista, a once-daily SGLT-1/2 dual inhibitor pill, for adults with type 1 diabetes. (For background on Zynquista, see here.) The FDA takes the committee’s vote into account as it decides whether to approve the drug. If approved, Zynquista could be the first pill approved for type 1s in the US, offering an additional therapy for A1C lowering, increased time-in-range, and weight loss. (In Europe, Forxiga may be approved for type 1 soon, following a positive recommendation from the European Medicines Agency.) Dr. Sherr did not find the tied vote discouraging: “a split vote is better than being denied.” JDRF believes there is a way to create steps to use SGLT inhibitors safely. There is potential, however, that the FDA might want to see more data on patient and healthcare provider education to reduce risk of diabetic ketoacidosis (DKA), the primary safety concern about using SGLTs in type 1. To help address this safety issue, we have created this infographic on precautions people might take to reduce the DKA risk, based on a consensus paper published in Diabetes Care.
On January 17th, an FDA Advisory Committee vote tied 8-8 on whether or not to approve Zynquista, a once-daily SGLT-1/2 dual inhibitor pill, for adults with type 1 diabetes. (For background on Zynquista, see here.) The FDA takes the committee’s vote into account as it decides whether to approve the drug. If approved, Zynquista could be the first pill approved for type 1s in the US, offering an additional therapy for A1C lowering, increased time-in-range, and weight loss. (In Europe, Forxiga may be approved for type 1 soon, following a positive recommendation from the European Medicines Agency.) Dr. Sherr did not find the tied vote discouraging: “a split vote is better than being denied.” JDRF believes there is a way to create steps to use SGLT inhibitors safely. There is potential, however, that the FDA might want to see more data on patient and healthcare provider education to reduce risk of diabetic ketoacidosis (DKA), the primary safety concern about using SGLTs in type 1. To help address this safety issue, we have created this infographic on precautions people might take to reduce the DKA risk, based on a consensus paper published in Diabetes Care.
In addition, Dr. Sherr also shared excitement for using Symlin, an injectable non-insulin treatment approved for both type 1 and type 2 diabetes, and Afrezza, an inhalable insulin. Dr. Kowalski is a believer in a Symlin-insulin combination for automated insulin delivery (AID) systems – Symlin reduces post-meal blood sugar peaks, which makes it well suited for automated insulin delivery. A recent study showed that the combination of insulin and Symlin increased time-in-range by nearly three hours per day (!) compared to insulin-alone AID systems. Afrezza is also being tested in combination with automated insulin delivery, helping to blunt the post-meal increase in blood sugar.
On Beyond A1C:
When speaking about her own experiences using Medtronic’s MiniMed 670G as a type 1, Dr. Sherr noted that her son said that she was “nicer” with the system. Dr. Kowalski shared that, while on a DIY system, his wife no longer had to wake up repeatedly due to low blood sugar CGM alarms. (Adam and Kelly have shared similar experience in their Loop test drives here and here.)
Considering these quality of life improvements, Dr. Kowalski emphasized the Beyond A1C movement, referencing the JDRF consensus statement published in Diabetes Care in 2017. In line with the core message of Beyond A1C, which emphasizes that A1C should not be the only outcome to measure how people with diabetes are doing, he urged the audience to think about “the benefit when you start to lift the burden a little off your shoulders.” Dr. Kowalski mentioned that even advances that might be perceived as small – such as using a smartphone to take a bolus, instead of pulling out a pump – can “impact life in a major way.” We completely agree – see here for our 2017 meeting on Beyond A1C when The diaTribe Foundation collaborated with ADA, AACE, Endo Society, FDA, JDRF, DSMA, and multiple other groups to discuss how to best show outcomes that affect patient well-being and success. (Here is a great video highlighting the importance of time-in-range!)
What an incredible opportunity for diaTribe to be present yet again at the Mission Summit. We thank JDRF for all that they do for the type 1 diabetes community – they are moving the needle in a major way on the future cures for type 1 diabetes.