Decoding Diabetes With Dr. Bob: Mental Health

Hear from Dr. Bob Gabbay, endocrinologist, researcher, and former Chief Scientific and Medical Officer of the American Diabetes Association, as he explores the most exciting topics and latest innovations in diabetes care.
I often find myself reflecting on the biggest challenges facing diabetes and how we might address them. This has been my nature for many years. Maybe it is my scientific mindset: Find a problem, identify the influencing factors, and strategically align on a solution. The frustrating aspect of diabetes is that there are many challenges, influencers, and certainly barriers to realizing solutions.
As I learned during my tenures at the ADA and Joslin Diabetes Center, strategic solutions are complex and often take time. Perhaps I am impatient! Progress, however big or small, is still progress, and the key is to keep chipping away at the issue – one step at a time.
This brings us to arguably one of the biggest challenges in diabetes: Mental health.
The diabetes mental health landscape
I can tell you from my continued clinical practice caring for people with diabetes that almost anyone with a high A1C undoubtedly faces mental health-related challenges. Even people with well-managed diabetes face the burden of diabetes stigma, guilt, frustration, anger, diabetes distress, and burnout. Mental health is consistently an area of diabetes care that is commonly forgotten by many healthcare professionals, yet is top of mind for people with diabetes.
While at ADA, we established a People With Diabetes (PWD) Council to guide research priorities. The resounding number one issue identified – beyond cures for type 1 and type 2 diabetes – was, in fact, mental health.
The challenge is that there are not enough mental health professionals available. To illustrate, despite the robust number of bachelor's degrees awarded in psychology each year (over 140,000 in 2023), the number of master’s and doctorate degrees awarded is much lower – around 38,000 and 7,200, respectively.
Mental health professionals with expertise in diabetes care are even more scarce. Within 100 miles of Boston, one of the larger metropolitan areas in the U.S. (and where I am based), the ADA’s mental health professional directory currently lists just 18 results. In the entire state of Nebraska, where Kelly Close (founder of Close Concerns and the diaTribe Foundation) grew up, that number is zero.
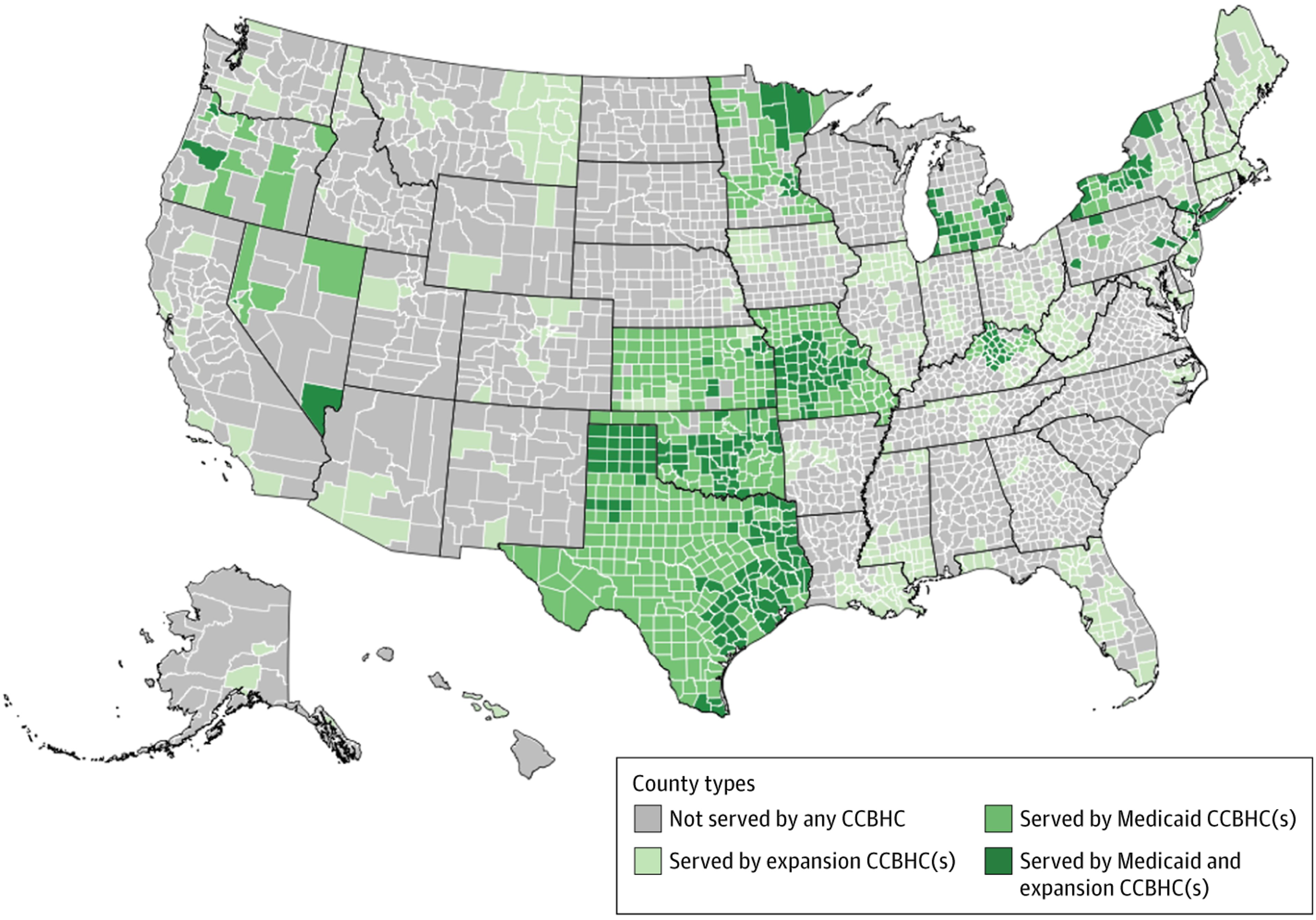
As shown below, many areas in the country are severely lacking in mental health services. As of June 2024, only 56% of the U.S. population resides in an area with a Certified Community Behavioral Health Clinic.
Why is there a shortage?
This shortage in mental health professionals is in part due to limited reimbursement available for their services. Most diabetes practices consider hiring mental health professionals a financial loss. The practices that do have them usually need to cross-subsidize or rely on philanthropy (as we did when I led the Joslin Diabetes Center) to support the necessary services. Sadly, this is not a sustainable or scalable business model.
In other cases where mental health services are available, underutilization is also an issue. Even the great Adam Brown, published author and brilliant therapist, has challenges filling his schedule.
From the provider side, underutilization can stem from limited referrals. Especially for providers who do not work in comprehensive and integrated care settings, it can be difficult to identify therapists. Furthermore, most therapists have limited knowledge of the challenges of diabetes.
For those with diabetes, access can be a barrier to seeking mental health services. People with diabetes may face potential out-of-pocket costs because mental health providers, who are already limited in number, often cannot make ends meet on low reimbursement rates from payers.
Stigma is another barrier to utilizing mental health services. People with diabetes may not want to see a therapist for fear of being treated differently or perceived negatively. It is also important to recognize that mental health stigma is more common in certain cultures. In many Asian cultures, for example, mental illness is often viewed as a sign of personal weakness and therefore is considered a taboo subject. Research shows that Asian people are less likely to seek mental health care compared to white people. Some people with diabetes may even experience “double stigma,” where they are stigmatized for having both diabetes and a mental health condition.
The solution?
What has been done and what can be done? To tackle the shortage of professionals with diabetes expertise while at the ADA, we partnered with the American Psychological Association and Helmsley Charitable Trust to establish a training program for mental health professionals and a directory of recognized providers.
Meanwhile, other healthcare professionals can be trained on how to deliver basic behavioral health services. Certified diabetes care and education specialists (CDCES) are a particularly valuable resource, and the ADA’s website also has a free behavioral health toolkit.
Teletherapy can potentially be effective for people with diabetes in areas with mental health professional shortages or who face mobility or transportation barriers. National organizations like the ADA, Breakthrough T1D, and diaTribe need to advocate for better reimbursement for these valuable services – both in-person and remote.
Increasing the conversation around mental health can help reduce stigma. For healthcare professionals, taking the first step by asking people with diabetes open-ended questions about how they are doing mentally can be helpful if they don’t feel comfortable bringing up the topic themselves.
And wouldn’t it be great if – along with the current coverage of an annual wellness visit for physical health – every person with diabetes also had an annual “well-being” check-in for their mental health? Importantly, this check-in should go beyond the surface and really engage people living with diabetes in conversation to understand deeply and assess the need for additional mental health care.
Getting there will require more evidence to build a strong business case, but in the meantime, continuing to raise awareness about mental health and discussing the topic openly can move us in the right direction.
So, what can we do now? If you are a healthcare professional, screen your patients for not only anxiety and depression, but also diabetes distress as outlined in the Standards of Care. Find out what mental health services exist in your area and refer your patients. When mental health professionals are limited, utilize CDCES referrals.
For all of us, take some deep breaths, treat yourself to something that charges your batteries, and continue to fight for the needs of those with diabetes.
The information and insights in this column are adapted from an original Closer Look column, published by Close Concerns. Written by Dr. Bob and Elaine Young, this column was originally designed for clinicians, researchers, and professionals working in diabetes and obesity care and has been adapted for diaTribe audiences.
Read the first installment of Decoding Diabetes With Dr. Bob here.