Diabetic Retinopathy vs. Diabetic Macular Edema: What's the Difference?

Key takeaways:
- Diabetic retinopathy (DR) and diabetic macular edema (DME) are related but separate eye conditions; one is a complication of the other.
- Both conditions are caused by prolonged high blood sugar levels, which lead to damage of the retina's blood vessels.
- For those living with diabetes, regular screening and close management of blood glucose can reduce the risk of developing either condition, preserving vision and preventing complications.
Diabetes that is not optimally managed puts one at risk for eye-related issues ranging from cataracts to retinopathy to glaucoma. In fact, it is the leading cause of blindness in people aged 18 to 64. With regular care and attention, however, many people with diabetes are able to protect their vision.
Diabetic retinopathy and diabetic macular edema are often mentioned in tandem, but they are not the same thing. Both diabetes-related eye conditions that affect blood vessels in the retina, the light-sensitive layer of nerve tissue in the back of the eye. Both can lead to vision loss and blindness if left unchecked. They are, however, two separate conditions with distinct characteristics, and understanding the distinctions, causes, risks, and symptoms, if any, of each condition is crucial for people with diabetes as well as for those involved in their care.
Diabetic retinopathy
A common complication of diabetes, diabetic retinopathy occurs when blood vessels in the retina of the eye are damaged or swollen, or begin to grow abnormally.
Anyone with type 1 or type 2 diabetes is at risk of developing diabetes-related retinopathy, and years of higher-than-recommended blood sugar levels can lead to damage and blockage of the tiny blood vessels in the retina, reducing blood circulation. When this blood supply is cut off, the eye tries to compensate by growing new blood vessels; however, these new blood vessels don’t properly develop and, especially in the later stages of the condition, begin to leak fluid, eventually leading to permanent vision loss.
“In the eye clinic, we see people with proliferative DR, a serious type of DR which can cause bleeding inside the eye, and people with non-proliferative diabetic retinopathy, an earlier type of DR. A person with proliferative DR may notice the bleeding inside the eye as more floaters in the eye,” said Dr. Rolake Alabi, MD, a vitreoretinal surgeon with Austin Retina Associates in Austin, Texas.
Signs of diabetic retinopathy
Early detection of DR can help preserve vision. While it may not have any symptoms, symptoms of diabetes-related retinopathy can include:
- Blurry vision
- Dark spots or eye floaters, which appear as small specks, strands, squiggles, cobwebs, or clouds that drift across one’s vision
- Difficulty seeing in low light conditions or at night
- Impaired color vision or difficulty telling the difference between certain colors
- Vision loss and, in severe cases, blindness
Risk factors for diabetic retinopathy

Having diabetes is itself one of the greatest risk factors for DR.
“The longer a person has diabetes, the more likely they will develop diabetic retinopathy,” said Dr. Steven Reed, O.D., President of the American Optometric Association.
That said, certain segments of the population living with diabetes have an even greater likelihood of developing diabetic retinopathy, so regular visits to an optometrist or ophthalmologist are even more critical. These include having medical conditions such as being pregnant, having high blood pressure or high cholesterol, or having a family history of the condition.
Race also can be a risk factor. “Hispanics and African Americans are at greater risk of developing diabetic retinopathy,” he said.
Treatment for diabetic retinopathy
Diabetes-related retinopathy is classified into four categories: mild, moderate, and severe (considered non-proliferative diabetic retinopathy), with the fourth classification being proliferative retinopathy.
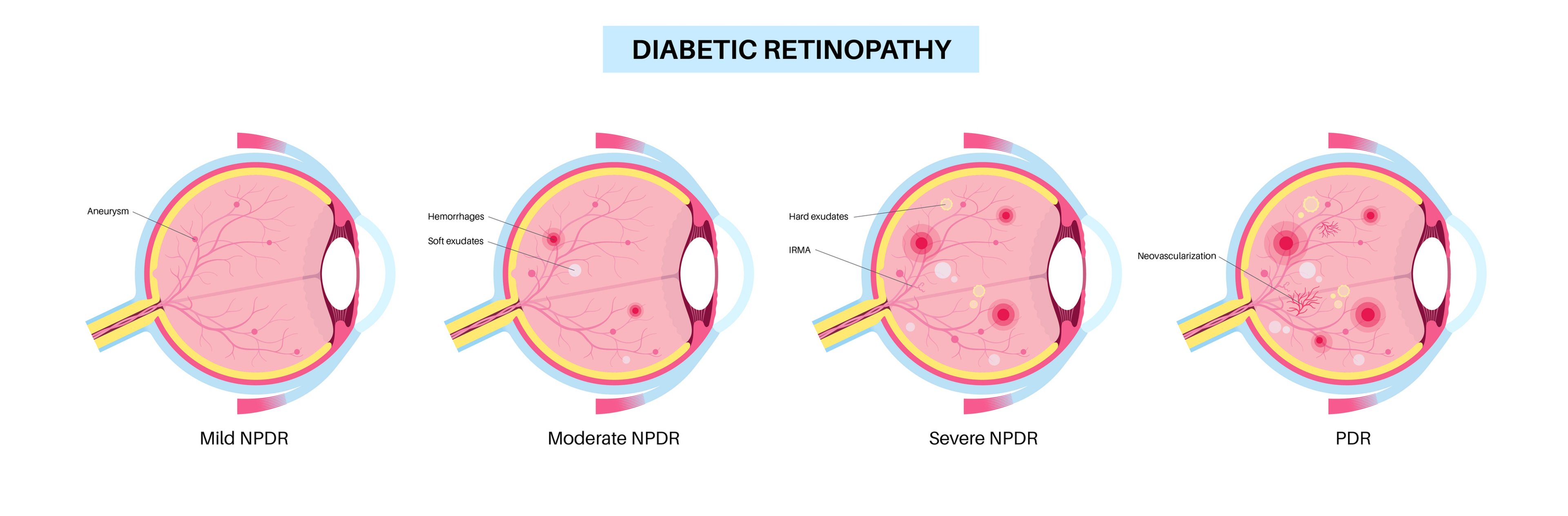
Treatment can vary depending on how far along the condition has progressed. Mild diabetic retinopathy, for instance, may simply require tighter blood glucose management to prevent progression and have visual improvement. Treatments such as laser therapy target leaking blood vessels or abnormal growth, while anti-VEGF injections block new vessels from forming and leaking, and steroid injections can be used to reduce swelling and abnormal vessel growth. In more advanced cases, a vitrectomy, a surgical procedure that removes the gel-like substance in the eye, may be required.
Regardless of how advanced one’s diabetic retinopathy is, blood sugar management should always be part of the equation, Alabi emphasized.
“Ideally, the best treatment is prevention. However, some patients also need eye treatment while they are working with their other doctors to control their blood sugars or if they have more difficult-to-control long-term DR complications.”
Diabetic macular edema
“Diabetic macular edema is a type of diabetic retinopathy caused by leakier than normal retinal blood vessels in some patients with diabetes,” Alabi said.

DME is a complication of diabetic retinopathy affecting a part of the retina called the macula. This 5 mm-wide layer located in the center of the retina is responsible for sharp, detailed vision.
When chronically high blood glucose levels reduce blood flow to vessels in the retina, the eye develops new but abnormal blood vessels that eventually leak fluid into the macula. As the macula accumulates fluid, it swells, leading to vision issues such as difficulty reading, recognizing faces, or seeing fine details. This is what’s known as diabetic macular edema.
Signs of diabetic macular edema
Because this condition affects the macula, or the part of the retina responsible for fine and detailed vision, diabetes-related macular edema often impacts one’s ability to notice fine visual detail. Symptoms of DME include:
- Blurred vision
- Difficulty reading fine print
- Difficulty recognizing familiar faces
- Distorted vision (straight lines that appear wavy)
- Dark spots or eye floaters, which appear as small specks, strands, squiggles, cobwebs, or clouds that drift across one’s vision
- Impaired color vision or difficulty telling the difference between certain colors
It is also possible to have DME without symptoms, according to Alabi.
“Many patients with DME will notice blurry or distorted vision, but it is possible to have DR and even DME that we see on eye examination and testing without significant visual symptoms or changes in the vision. This is one reason it is important to come in for regular eye examinations.”
Treatment for diabetic macular edema
First-line DME treatment involves healing the retina through the use of anti-VEGF medications, injection-based therapies that block the effects of vascular endothelial growth factor (VEGF), a protein that causes abnormal blood vessel formation and leakage.
If anti-VEGF injections are not fully effective or need to be spaced out, treatment may also involve steroid injections to reduce swelling. Macular laser therapy, while less commonly used as a first treatment today, is still used, and targets leaking blood vessels by sealing them to reduce fluid leakage and swelling. In advanced cases where there is severe scar tissue or retinal detachment, one may need a vitrectomy, a surgical procedure that removes the gel-like substance in the eye.
In addition to these treatments, DME treatment also involves treating the underlying cause of the eye complication: years of higher-than-ideal blood sugar levels.
Understanding the difference between diabetic macular edema and diabetic retinopathy
While not identical, DR and DME are closely related. Diabetic retinopathy refers to damage to the blood vessels in the retina, which can cause vision problems over time. Diabetic macular edema, on the other hand, is a complication of DR that happens when retinal fluid builds up in the macula, leading to swelling and causing vision impairment.
DME can occur at any stage of DR, including nonproliferative diabetic retinopathy (NPDR), which occurs at an earlier stage of DR. While DR is the broader term that encompasses various stages of retinal damage caused by diabetes, DME is a particular manifestation that occurs in the later stages of DR and is characterized by edema (swelling) in the macula.
Can one have diabetic retinopathy without diabetic macular edema?
Yes. While diabetic macular edema can develop as a result of advanced diabetes-related retinopathy, it is possible for someone to have diabetic retinopathy without also having diabetic macular edema. While DME can occur at any stage of diabetic retinopathy, the condition is more common in the later stages of DR.
Can one have diabetic macular edema without diabetic retinopathy?
Since diabetic macular edema is a complication of diabetic retinopathy, it is not possible to have DME without having DR. There are, however, other types of macular edema that are not caused by diabetes, so it is possible to still have macular edema without diabetic retinopathy or without having diabetes at all.
“Macular edema can develop from several conditions aside from unmanaged diabetes including retinal vein occlusion, inflammatory eye disease, age-related macular degeneration, hereditary disorders and other eye surgeries or trauma,” Reed said.
“Identifying the specific cause of macular edema is crucial,” he said. “This is why it’s important to schedule yearly comprehensive eye exams with your doctor of optometry and not to hesitate in booking an appointment when you are feeling something is off.”
Understanding DR and DME: The bottom line
Diabetic macular edema and diabetic retinopathy are two major eye conditions associated with diabetes, and while they are closely connected, they are not the same thing. Diabetic retinopathy refers to damage of the blood vessels throughout the retina, while diabetic macular edema refers specifically to swelling in the central part of the retina called the macula, which is responsible for seeing fine details.
Though they are connected, DR and DME can occur independently. Diabetes-related macular edema can develop as a result of advanced diabetes-related retinopathy, but it is possible for someone to have diabetic retinopathy without also having diabetic macular edema.
The best way to both prevent and manage either eye condition, Alabi said, is through close blood sugar management and vigilant diabetes management as well as regular eye screening exams to ensure timely treatment for any early signs of eye damage.
“Good control of blood sugars and blood pressure can help with prevention of DR and help with making the treatments of DR we offer in the eye clinic as effective as possible.”
Learn more about diabetes-related eye health:
- How to Keep Your Eyes Healthy With Diabetes
- Diabetic Macular Edema: How I Almost Went Blind
- Diabetic Macular Edema Treatment: What’s the Future?
Photo credits: iStock (top, middle); courtesy American Optometric Association (top headshot); courtesy Austin Retina Associates (bottom headshot).