Decoding Diabetes With Dr. Bob: Automated Insulin Delivery

Hear from Dr. Bob Gabbay, endocrinologist, researcher, and former Chief Scientific and Medical Officer of the American Diabetes Association, as he explores the most exciting topics and latest innovations in diabetes care.
Automated insulin delivery (AID) is a remarkable development in diabetes care. For those less familiar, AID systems – also known as hybrid closed-loop or “artificial pancreas” systems – automatically adjust insulin delivery based on glucose levels. They consist of a continuous glucose monitor (CGM), an insulin pump, and an algorithm/software that uses CGM output to adjust insulin dosing in real time.
While current systems still have a long way to go to be fully closed-loop systems (i.e., no meal content and announcements or adjustment for exercise), things are much better now than they were just a decade ago. In comparison to cars, people with diabetes are now in the equivalent of a semi-automatic car.
Future systems might elevate the experience from a basic sedan to a sports self-driving car equivalent – we can’t wait until the technology advances even further, though we appreciate all that these systems have done thus far for people with diabetes.
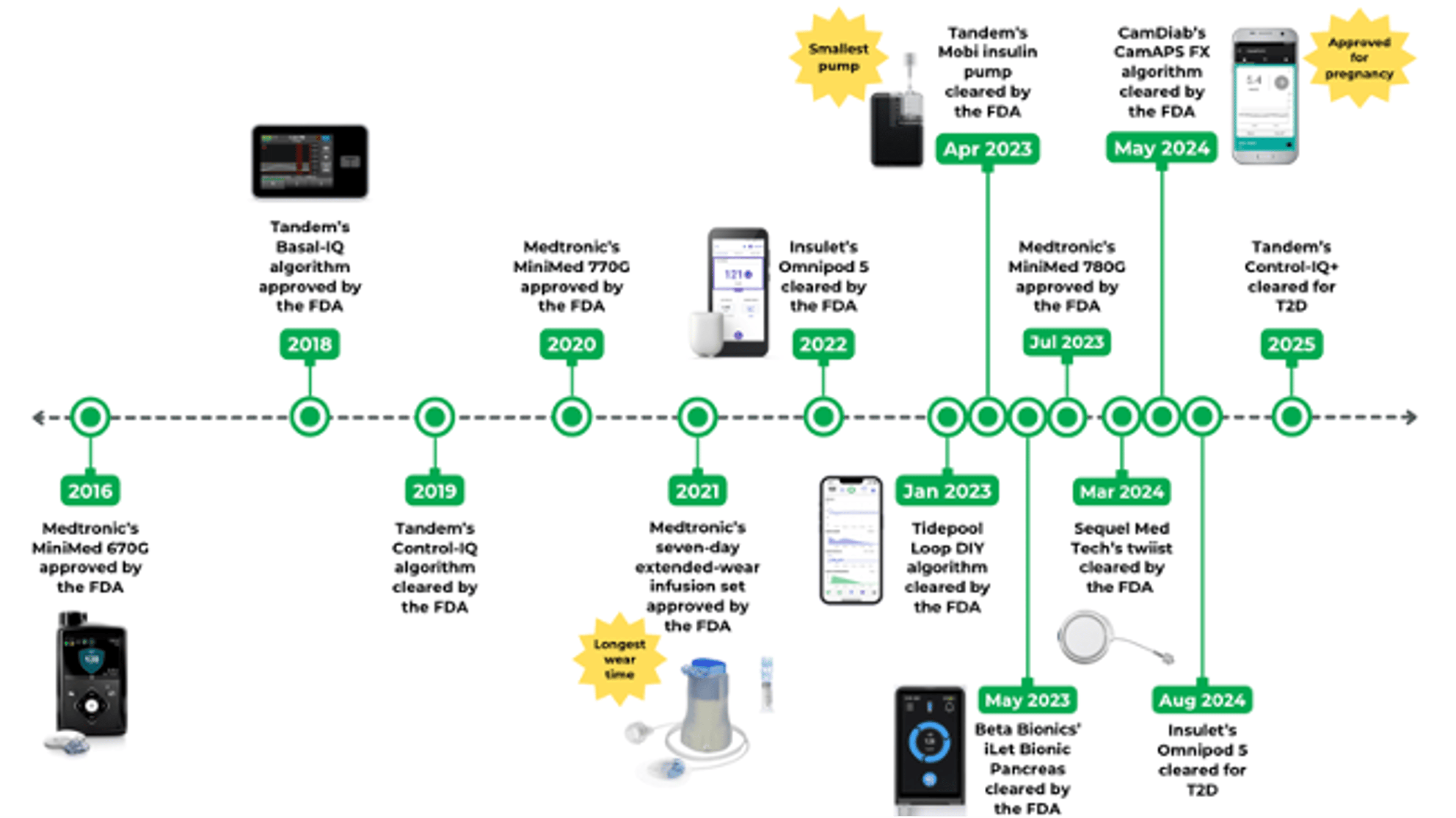
Automated insulin delivery: 2016 to present day
AID systems first became available less than 100 years after the discovery of insulin in 1921. The open source OpenAPS system launched in 2015, followed by the FDA approval of Medtronic’s MiniMed 670G in 2016.
Since then, multiple AID and pump manufacturers have brought their systems to market, including:
- Medtronic’s latest system, the MiniMed 780G
- Tandem’s t:slim X2 and its newer Mobi product – currently the smallest AID system on the market
- Insulet’s tubeless Omnipod 5
- Beta Bionics’ iLet Bionic Pancreas, which eliminates the need for accurate carb counting
- Sequel Med Tech’s twiist, which offers precise microdosing
How many people use AID?
The number of people using AID globally is growing rapidly, with 300,000 new users in 2024 alone.
While AID users are primarily those with type 1 diabetes, a sizeable and growing number of people with type 2 diabetes also appear to be interested in this technology, particularly those who find difficulties using multiple daily injections (MDI). Uptake is likely to increase among people with type 2 diabetes, given the approval of two AID systems for this population – the Omnipod 5 and Tandem’s Control-IQ+ – with other manufacturers in the process of seeking type 2 diabetes indications as well.
These numbers suggest that there are millions of people globally who could benefit from being on an AID system but aren’t on one currently, which I consider a missed opportunity.
Why should more people be on AID?
Broadly speaking, diabetes technologies have been shown to improve clinical and psychosocial outcomes while also reducing healthcare costs and resource utilization. With AID, multiple studies have demonstrated the technology’s cost-effectiveness and positive impact on quality of life.
One key benefit of AID is its ability to significantly reduce (or even eliminate) episodes of severe hypoglycemia. Research has found that AID is an effective tool to help people with diabetes reach the recommended time in range (70-180 mg/dL) goal of 70%. At the Joslin Diabetes Center, I have a patient who has had diabetes for over 50 years and has had frequent hypoglycemia. It took a while to get him on board with AID, but once he was on it, he loved it. AID improved his self-management significantly.
Part of the issue was “trusting” the autonomous nature of the system – for folks who have had to pay particular attention to all aspects of their management for decades, it can be hard to let go of that kind of control. For those without diabetes, I would compare it to the first time I rode in a driverless Waymo car in San Francisco. After some hesitation, I was able to yield to an autonomous system to drive me around, depending on external decisions for safety.
Severe hypoglycemia has been the principal constraint to the use of insulin since its discovery, given potentially fatal outcomes when misused. As Jim Hirsch points out in his article on the evolution of insulin pumps and his experience using AID, “remove severe hypoglycemia as a threat, and you change the course of type 1 diabetes.” This hints at the key potential of AID and why broader adoption is so important.
Does insurance cover AID systems?
U.S. coverage falls under one of two cost models: pharmacy benefits or durable medical equipment (DME):
- With pharmacy benefits, patients can go to their local pharmacy for their pumps. Currently, this model mostly applies to patch pumps and the twiist pump, since they are disposable and relatively low-cost.
- DME benefits, by contrast, apply to AID systems such as MiniMed 780G and t:slim X2, which have larger, reusable pumps with disposable cartridges. This model often requires patients to pay a significant upfront cost to purchase the pump. Additionally, patients are required to go directly through DME companies, which can be challenging and time-consuming to work with, given their range of product availability besides insulin pumps. For healthcare providers, using the DME channel also often means a lot more paperwork. The good news is there is movement to have more pumps available through pharmacies.
What are current barriers to AID adoption?
AID adoption has continued to grow, yet remains challenging for numerous reasons. Access is a big one. In countries where AID is available, cost can be a significant barrier. As you can see above, in the U.S., payer coverage for AID systems can vary, with particular gaps in Medicaid.
Other barriers to adoption include the perceived complexity of AID systems and resistance to change, or a lack of trust in technology. Some patients may also feel that AID systems have not progressed enough to full automation. For example, most AID systems still require carbohydrate counting, and manual workarounds may also be necessary for certain scenarios, such as exercise, flying, and pregnancy.
Others may have tried AID but, perhaps due to a lack of support or education, stopped using it because it became more of a burden than a helpful tool for managing their diabetes. For instance, I had a patient who has had diabetes for a long time and is generally good about self-management. They were on a pump for a few years, but didn’t trust AID. When they started using it, they would take it out of auto mode quite often. Eventually, with some more experience and coaxing, they got comfortable with letting it run on autopilot and now love it – and it’s given them some of their life back from not needing to constantly obsess over their numbers.
The CamAPS FX system, though recently approved for use during pregnancy, is not yet commercially available in the US due to the absence of a compatible insulin pump partner. Features such as pump waterproofing, size, and battery life are also important practical considerations for patients.
Getting healthcare providers on board
Another issue is that many primary care providers lack familiarity with AID use but don’t have time to fit expanded diabetes technology into their busy workflow. Multiple appointments are generally required for AID training, which frequently results in scheduling constraints. Many providers do not have certified diabetes care and education specialists (CDCES) available to help onboard patients and troubleshoot.
One persistent barrier is carbohydrate counting – a process that's often unfamiliar to primary care providers and their staff, and burdensome for many patients. Here too, startups are stepping in. Companies like Inreda and CamDiab, along with several others, are offering tools that claim to have solved this problem entirely.
Providers also need to dedicate time to navigate insurance approval (e.g., prior authorization, coverage criteria) on their own. Contrast this with Joslin, where multiple technology coordinators help navigate coverage and onboarding for patients – this is not scalable or affordable for most primary care providers.
Addressing these challenges will likely involve offering free or low-cost training for continuing education credit, simplifying diabetes technology even more, and standardizing the initiation process.
For training, ADA, for example, offers free courses and webinars. Another is Project ECHO, a great model to equip healthcare providers and their teams with the tools and knowledge to deliver high-quality care to people with diabetes.
These scenarios also highlight the importance of patient education and support models. Given the endocrinologist shortage, leveraging CDCES will be key for this effort. Another idea to expand adoption may be to utilize pharmacists, who could be taught to analyze data and work with AID users directly.
What’s next for AID?
We are approaching a decade since the first AID system was approved, and there have been many advancements since then.
Most notably, pumps have gotten smaller, children as young as 2 years old can now use AID, and infusion sets can be worn for up to seven days instead of three. The guidelines have changed, too – the ADA recommends offering AID to anyone with type 1 diabetes, even early after diagnosis.
What can we potentially look forward to in the next few years?
Fully closed-loop systems
The dream, I argue, would be a fully closed-loop system in which no engagement is needed from the user. There are research groups like UVA and other companies actively working on such systems.
With all the promising data coming out on fully closed-loop systems, I think we are getting closer to seeing some of these systems approved and commercially available. Beyond the clinical benefits, the psychosocial benefits of such a system would likely be incredible.
Imagine a world where all you had to do was put on an AID every few days, and it would run automatically in the background, and you would not need to do anything. A fully closed-loop system would be even easier to start and use – a key to getting more people with diabetes and primary care providers on board with offering AID to their patients (plenty already are!). I even have some patients on non-commercial fully closed-loop systems who are doing very well with no meal announcements.
New players in the field
While the market is currently dominated by three major public companies (Insulet, Medtronic, and Tandem), smaller – and possibly nimbler – companies are emerging as potential contenders.
For example, Beta Bionics and its AID system, the iLet Bionic Pancreas, is arguably the simplest system available. It only requires the user’s body weight to start, and during meals, the user only needs to estimate their meal size (i.e., more than usual, usual, or less than usual) – no carbohydrate counting or insulin-to-carbohydrate ratios.
Sequel Med Tech (co-founded by Dean Kamen, the inventor of the first commercially available insulin pump) will be testing uncharted waters, announcing just recently that it plans to integrate its twiist AID system with Senseonics’ one-year implantable CGM, Eversense 365, and Abbott’s upcoming dual glucose-ketone sensor.
What is exciting about newer companies is that they are often hyper-focused on specific innovations. For instance, Beta Bionics and Dutch company Inreda are developing bi-hormonal AID systems that deliver both insulin and glucagon, while Sequel is working on faster occlusion detection with twiist.
Luna Diabetes is currently developing a simple nighttime AID system that addresses the challenge of overnight blood sugar management. This offers the added benefit of not needing to wear something during the day – for some individuals, perhaps more often with younger folks, this also means avoiding unwanted attention and stigma.
One company, PharmaSens, is also working on a system combining a CGM and an insulin pump in one wearable. Many of these new players are scrappy startups, and they are worth watching. They are determined to tackle big problems, often with limited funds.
Concluding thoughts
AID technology has come a long way since the first commercial system was approved in 2016. Since then, the field has been hard at work innovating, making AID systems significantly smarter, smaller, simpler, more affordable, and safer.
What we need now is more people with diabetes – anyone with type 1 diabetes or insulin-treated type 2 diabetes – to be offered this highly effective therapy that both improves outcomes and helps with the management of the constant burden of living with diabetes.
As healthcare providers become more tech savvy with AID systems and as devices become simpler and more autonomous and better at adjusting to individual users, AID adoption is likely to continue to grow.
The information and insights in this column are adapted from an original Closer Look column, published by Close Concerns. Written by Dr. Bob and Elaine Young, this column was originally designed for clinicians, researchers, and professionals working in diabetes and obesity care and has been adapted for diaTribe audiences.
Read more installments of Decoding Diabetes With Dr. Bob here: