Your A1C May Not Be Reliable If You Have Chronic Kidney Disease

Key takeaways:
- Diabetes is a leading cause of chronic kidney disease, a condition where kidneys gradually lose their ability to function over time.
- Chronic kidney disease can lead to inaccurate A1C readings due to anemia and changes in red blood cell production, which may make A1C unreliable for blood sugar monitoring.
- Alternative solutions, such as continuous glucose monitoring and time in range, may offer more accurate insights into blood glucose management.
Chronic kidney disease is a major complication associated with diabetes that can lead to inaccurate A1C measurements, especially in advanced stages. We’ll explore why this is and what you can do to manage your blood sugar if you have kidney disease.
According to the Centers for Disease Control and Prevention (CDC), diabetes is one of the leading causes of chronic kidney disease, also referred to as diabetic kidney disease. Other risk factors include high blood pressure, a family history of kidney disease, obesity, and heart disease. Approximately one in three adults with diabetes may have chronic kidney disease, and many are unaware they have it. Because early-stage kidney disease often presents without symptoms, it’s important to get your kidney health checked regularly. Healthcare professionals use a combination of urine and blood tests to check kidney function.
Treatment for diabetic kidney disease also involves treating the underlying cause: chronically high blood glucose levels. A1C is an important measurement used to assess overall diabetes management and risk for complications, but it does have some limitations. Since A1C is one value that estimates glucose levels over the preceding two to three months, it doesn't provide details about daily glucose trends or inform about hypoglycemia (low blood sugar). When someone has chronic kidney disease, the accuracy of their A1C values can be compromised.
It is important to talk with your healthcare provider about some of the challenges and limitations of A1C to know which method of blood glucose monitoring is right for you. You can discuss supplementary measurements, such as time in range using continuous glucose monitoring (CGM), with your healthcare team.
What is chronic kidney disease and how does it relate to diabetes?
The kidneys are important organs in our body responsible for several essential functions, including:
- Removing waste products from the blood and other body fluids
- Balancing the fluids and salts in the body
- Helping manage blood pressure
- Activating vitamin D, which helps keep bones healthy
- Helping make hormones that stimulate bone marrow to make red blood cells
Chronically high blood sugar levels, along with high blood pressure, can damage the kidney’s small blood vessel filtering system and lead to kidney failure.
For most people with chronic kidney disease, standard treatment is focused on slowing the progression of the disease with lifestyle modifications and blood pressure-lowering medications. However, recent studies have shown that treatment with SGLT-2 and GLP-1 medications, which help lower blood glucose, provides additional kidney and heart benefits. This is especially true for people with diabetes, although it is important to note that SGLT-2 medications are not approved by the FDA for individuals with type 1 diabetes. In recent years, SGLT-2 medications have been added to treatment guidelines as a key disease-modifying therapy for individuals with type 2 diabetes and chronic kidney disease.
How does chronic kidney disease affect A1C in people with diabetes?
Recent studies have shown that A1C, as a measure of blood glucose management, may be less accurate for people with chronic kidney disease, especially those with advanced chronic kidney disease (this means kidney function or eGFR less than 30) or who are on dialysis.
A1C measures the amount of glucose bound to hemoglobin in red blood cells over time. In chronic kidney disease, higher levels of waste products in the blood can affect the way glucose binds to these red blood cells. Since A1C measurements depend on both blood sugar levels and red blood cell lifespan, declining kidney function may cause A1C measurements to be unreliable.
Some reasons why chronic kidney disease may overestimate or underestimate a person’s actual A1C are illustrated in the KDIGO clinical practice guidelines. In some cases, chronic kidney disease can lead to an A1C that appears higher than it actually is. For example, when the kidneys begin to fail, they are unable to remove acids that build up in the body. This buildup of acids (labeled “metabolic acidosis” in the figure) speeds up the process of glucose binding to hemoglobin, causing A1C to appear to be higher even if your blood glucose is actually lower.
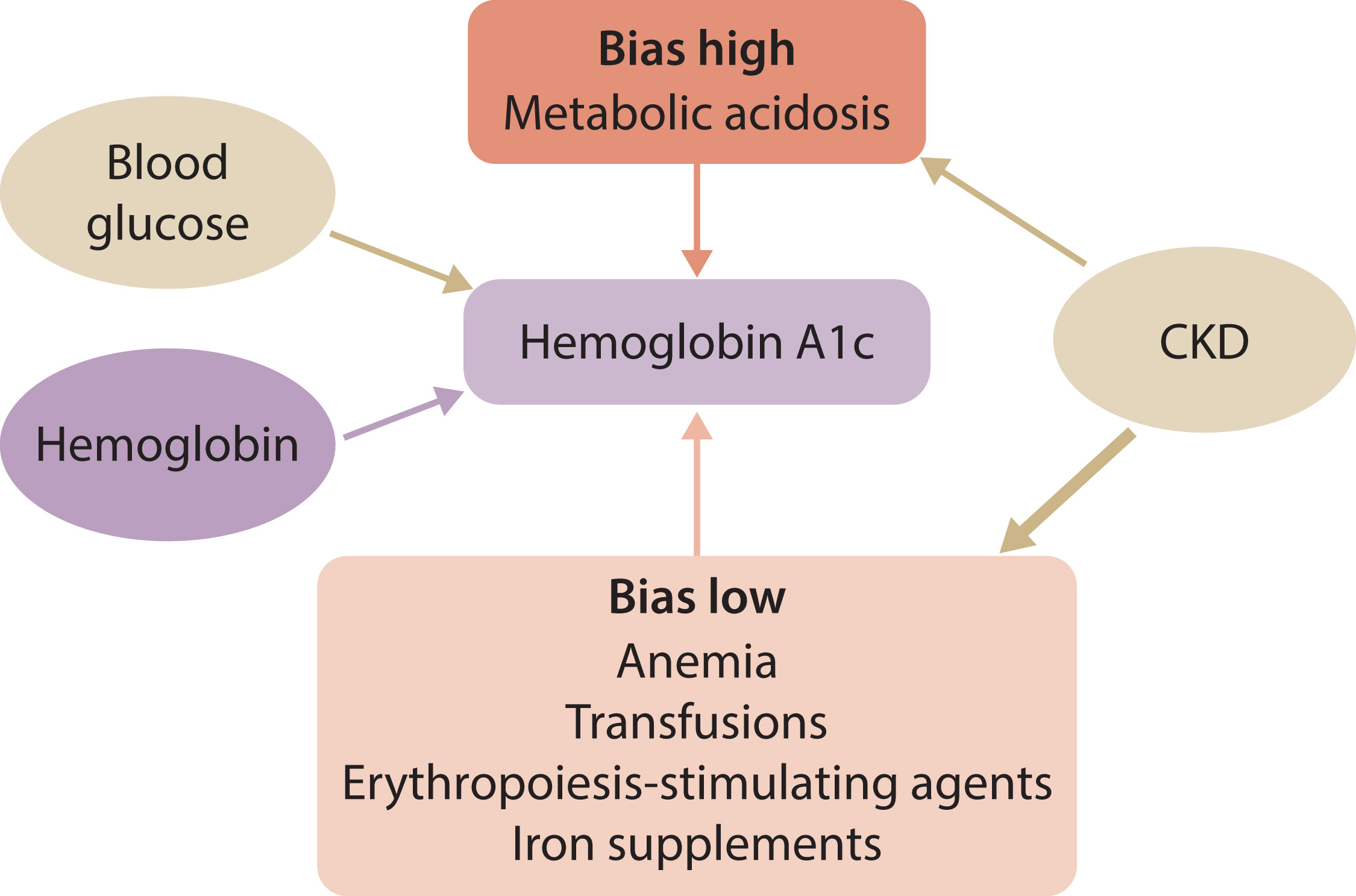
On the other hand, chronic kidney disease can also lead to an A1C that is seemingly lower than it actually is. That’s because kidney disease can reduce red blood cell production, leading to anemia (a lower-than-normal red blood cell count). This means that there is less hemoglobin for glucose to bind to, which makes A1C appear to be lower, even if your blood glucose really is higher.
Additionally, blood transfusions and medications that help your body to make more replacement red blood cells can have the same effect. Therefore, if you have a diabetes diagnosis and are at risk of developing kidney disease, it is critical that you discuss your A1C target with your healthcare team.
Ask your healthcare team about using diabetes technology like CGM and automated insulin delivery (AID) systems, which can help you keep track of and manage blood sugar levels.
How can blood sugar management be improved for people with diabetes and chronic kidney disease when A1C is not reliable?
While clinical practice guidelines still recommend using A1C to monitor blood sugar management in people with diabetes and chronic kidney disease, they recognize the limitations of A1C among those with chronic kidney disease.
Supplementing A1C with other measures of blood glucose management, such as time in range, may help paint a more accurate picture of an individual’s blood glucose status. CGM can also help people monitor hypoglycemia by measuring time below range – a particular risk as the kidneys fail and break down less insulin.
Further research on using CGM as a supplement to A1C is needed to help us better understand how people with diabetes and chronic kidney disease can improve their blood sugar management.
Learn more about chronic kidney disease and diabetes here:
- Predicting Kidney Disease in People with Diabetes
- Chronic Kidney Disease: The Hidden Complication
- Limitations of A1C: How Does A1C Vary by Race and Ethnicity?
Photo credit: KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease